Research Article - Journal of Clinical Ophthalmology (2025) Volume 9, Issue 1
Wedge technique for corneal lenticule extraction in refractive surgery.
Gitansha Shreyas Sachdev*
Department of Ophthalmology, The Eye Foundation, Coimbatore, India
*Corresponding Author:
- Gitansha Shreyas Sachdev
- Department of Ophthalmology, The Eye Foundation, Coimbatore, India
- E-mail: sachdevgitansha@gmail.com
Received: 22-Nov-2024, Manuscript No. AACOVS-24-153114; Editor assigned: 27-Nov-2024, AACOVS-24-153114 (PQ); Reviewed: 11-Dec-2024, QC No. AACOVS-24-153114; Revised: 08-Feb-2025, Manuscript No. AACOVS-24-153114 (R); Published: 15-Feb-2025, DOI: 10.35841/aacovs.9.1.502
Citation: Sachdev GS. Wedge technique for corneal lenticule extraction in refractive surgery. J Clin Ophthalmol. 2025;9(1):502
Abstract
Corneal lenticule extraction based procedures are the latest advancement in the field of keratorefractive surgery. Difficulties in lenticule extraction with pursuant complications like piecemeal removal and remanent lenticular fragments, corneal side cut or cap tear, may have an increased incidence in the hands of a novice surgeon or in low myopic correction with thin lenticules. These complications can be avoided by optimizing machine energy parameters and ascertaining complete lenticule separation prior to attempted removal. We describe a novel technique for lenticular dissection, to facilitate complete separation and smooth extraction. In this technique, a small tissue wedge is left undissected during the posterior lenticule separation, allowing adequate counter resistance to maintain lenticule fixation without undesired movements and complete subsequent separation. We performed this technique in 250 eyes of 129 patients and complete lenticule separation was achieved in all eyes.
Keywords
Small incision lenticule extraction, SMILE, Corneal lenticule extraction for advanced refractive correction, CLEAR, Lenticule.
Introduction
Lenticule extraction techniques including Small Incision Lenticule Extraction (SMILE) and Corneal Lenticular Extraction for Advanced Refractive correction (CLEAR) are the latest additions in the armamentarium of the refractive surgeon. Numerous publications have reported similar safety, efficacy and predictability of refractive outcomes vis-a-vis Femtosecond Laser-Assisted Keratomileusis (FS-LASIK) [1,2].
Lenticular extraction procedure entails docking, femtosecond laser application for the creation of the intrastromal lenticule, separation of the lenticule from surrounding stroma and subsequent extraction via a corneal side cut incision. Manual extraction of the lenticule must be done with utmost care, as if not performed appropriately, may result in complications. Different modifications of the surgical technique have been described to ease the process of lenticule dissection and extraction to minimize complications [3-6]. We describe a novel technique for lenticular dissection, to facilitate complete separation and smooth extraction.
Materials and Methods
Study population and design
This interventional study was conducted at a tertiary eye care hospital in South India. Written informed consent was taken from all participants in accordance with the tenets of
Declaration of Helsinki, and an Ethics committee approval was obtained.
The study included patients with age greater than 18 years and a stable refractive error (change in Manifest Refractive Spherical Equivalent (MRSE) of not more than 0.25D over one year), undergoing SMILE or CLEAR for refractive correction. Soft and rigid contact lenses were discontinued 1 and 3 weeks prior to corneal tomography.
Exclusion criteria were as follows: Eyes with inadequate preoperative pachymetry (less than 500 microns) or residual stromal bed post lenticule extraction of lower than 280 microns, corneal tomographic abnormalities including keratoconus or pellucid marginal degeneration, corneal scars, pregnancy and ocular comorbidities.
Following investigations were performed at preoperative and sixweeks postoperative visit: Uncorrected (UDVA) and Corrected Distance Visual Acuity (CDVA) measurement, subjective refraction, slit lamp bio microscopy, fundus evaluation and corneal tomography (Pentacam, Oculus, Optikgerate, Gmbh).
The lenticule extraction technique was performed using either of the two femtosecond laser platforms: Small Incision Lenticule Extraction (SMILE) was carried out on the Visumax laser system (Carl Zeiss Meditec, Germany) and Corneal Lenticule Extraction for Advanced Refractive correction (CLEAR) was performed on the Femto LDV Z8 (Ziemer). All surgeries were performed by a single experienced surgeon with greater than 10 years of refractive surgery experience and subsequently 7 refractive surgeons were trained with the same technique. The ease of surgical dissection and lenticule removal and the incidence of lenticule folding over or incomplete lenticule separation was assessed by the surgeons. The presence of lenticule adhesions or remanent lenticular fragments, if any, were noted.
Postoperative medication regimen included steroid eye drops (L-pred 0.5%) in tapering dose over one month, eye drops moxifloxacin 0.5% (Vigamox) four times a day for one week and lubricant eye drops (Systane Ultra) four times a day for 3 months.
Surgical technique
The procedure is carried out under topical anesthesia using aseptic precautions. Following a proper dock with precise centration, four cleavage planes are created by the femtosecond laser including the posterior lenticule cut, lenticule side cut, anterior lenticule cut and the corneal side cut. Additionally, posterior and anterior corneal venting incisions are created on the CLEAR platform.
The corneal side cut is opened by entering vertically using a sharp tipped instrument. The anterior and posterior lenticule plane is subsequently delineated. The stop sign allows correct identification of the planes by utilizing the resistance to lateral movement noted at the junction of the dissected and undissected halves [3]. The anterior cleavage plane is enlarged and the dissection of the anterior lenticule surface is completed end to end. The wedge dissection technique allows ease while dissecting the posterior lenticular plane. The dissector is introduced into the posterior cleavage plane and the dissection is completed all the way till the inferior end. The inferior lenticule dissection is completed on the surgeons left (6 to 4 o’clock) and the right side (6 to 8 o’clock) respectively. Superior lenticule dissection on the left is completed (2 to 12 o’clock) after leaving behind a triangular wedge shaped undissected tissue (4 to 2 o’clock). Subsequently, the dissection of the superior lenticule on the surgeon’s right is completed fully (8 to 12 o’clock) (Figure 1). The undissected wedge allows counter traction during this stage. This prevents rolling or folding over of the free dissected area which usually complicates further dissection. The wedge is finally dissected and the separated lenticule is subsequently removed using micro forceps. The integrity of the lenticule is evaluated to rule out any residual fragments left in the pocket. This technique enables an easy and safe extraction while avoiding excessive lenticule movement and associated difficulties in subsequent dissection.
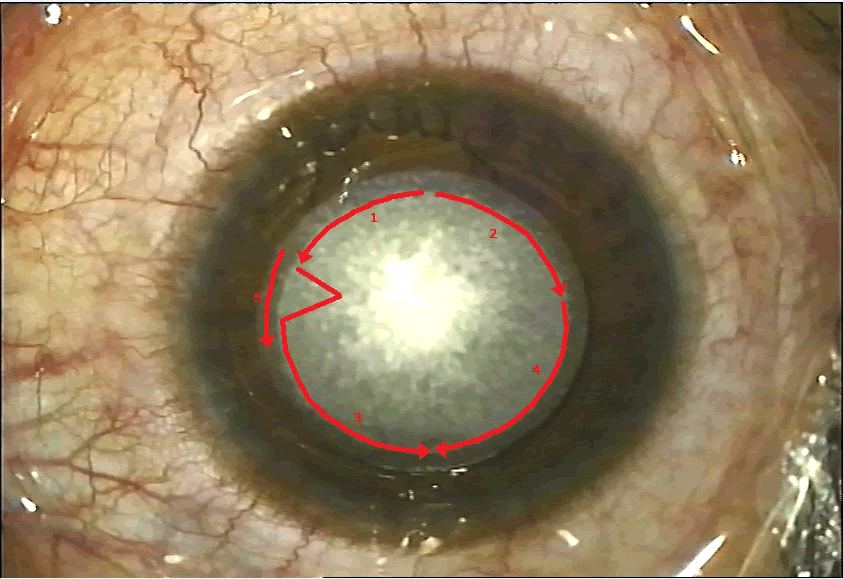
Figure 1. Steps for posterior lenticular plane dissection 1) Completed up till the lenticular side cut from 6 to 4 o’clock position, 2) Followed by 6 to 9 o’clock, 3) A wedge shaped undissected tissue is left undissected following which remaining superior dissection is competed from 2 to 12 o’clock, 4) and 9 to 12 o’clock, 5) Triangular wedge is finally dissected.
Results
Two fifty eyes of 129 patients underwent corneal lenticular extraction using the wedge dissection technique. The surgeries were performed by a single experienced surgeon with greater than 10 years of refractive surgery experience and subsequently 7 refractive surgeons were trained with the same technique. The mean spherical equivalent treated was -2.35 ± 0.65 Diopter, with a mean lenticule thickness of 54.65 ± 12.10 microns. There were no reported incidents of lenticule folding over and a complete separation was achieved in all eyes. There were difficulties in lenticule extraction in five eyes as the wedge dissection was not fully completed before attempted removal. However, subsequent to complete dissection, lenticule removal was achieved. No remanent lenticule fragments were observed and a complete lenticule was ascertained upon removal. None of the surgeons experienced any difficulties in surgical maneuvers.
Discussion
Corneal lenticular extraction techniques allow refractive correction without the construct of a flap, thereby affording greater biomechanical stability and reduced incidence of dry eye. However, the learning curve is longer and unique complications associated with difficult lenticule extraction have been described [7,8]. Various techniques have been published for efficient lenticule removal and improved surgical outcomes. Chungs swing technique [4] and lenticulorhexis [5] demonstrated incidence of incomplete lenticule separation and torn lenticular fragments, especially in low myopic correction with thinner tissue. The sequential segmental terminal lenticular side-cut dissection described by Jacob and colleagues [6], entails central dissection of the posterior plane while sparing a thin peripheral rim till the end. However, difficulties in the final segment dissection with use of lenticulorhexis technique in some cases has been mentioned. The final intact segment includes the right superior rim located under the corneal side cut incision. Our technique overcomes this limitation by placing the wedge at a more ideal location (central left quadrant for a right handed surgeon) permitting ease of surgical manipulation. Additionally, creation and subsequent dissection of a single undissected wedge as against multiple segments, would be less time consuming and easier to perform. The intact wedge allows fixation of the lenticule till the very end without undesired movements, enabling a smooth and complete dissection.
The position of the wedge is on the left hand side for a right handed surgeon and vice-versa. Additionally, the placement is along the horizontal plane as against sub incisional in the technique described by Jacob. Both these factors attribute to greater surgical ease and manoeuvring. The width of the wedge is two clock hours, allowing adequate anchoring even in thin lenticules which may spontaneously separate along the cleavage lines. Additionally, it is not too large so as to require excessive dissection and manipulation at the last step, resulting in undesired movement of the dissected lenticule.
With an increased incidence of lenticule extraction procedures, a well-defined technique of lenticule dissection affords more consistent outcomes, especially while training novice surgeons. Visually significant complications such as retained lenticular fragments and delayed visual recovery secondary to excessive surgical manipulation can be avoided.
Conclusion
In conclusion the wedge technique for lenticular dissection is effective for all refractive power corrections and allows safe surgical extraction even in the hands of a novice surgeon.
Financial Disclosure and Conflict of Interest
Nil.
References
- Titiyal JS, Kaur M, Shaikh F, et al. Small Incision Lenticule Extraction (SMILE) techniques: Patient selection and perspectives. Clin Ophthalmol. 2018;12:1685-99.
[Crossref] [Google Scholar] [PubMed]
- Guo H, Hosseini-Moghaddam SM, Hodge W. Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: A systematic review and meta-analysis. BMC Ophthalmol. 2019;19:167.
[Crossref] [Google Scholar] [PubMed]
- Sachdev GS, Ramamurthy S, Dandapani R. Stop sign for correct tissue plane identification in small incision lenticule extraction. Indian J Ophthalmol. 2020;68:895-6.
[Crossref] [Google Scholar] [PubMed]
- Kim BK, Mun SJ, Lee DG, et al. Chung’s swing technique: A new technique for small-incision lenticule extraction. BMC Ophthalmol. 2016;16:154.
[Crossref] [Google Scholar] [PubMed]
- Zhao Y, Li M, Yao P, et al. Development of the continuous curvilinear lenticulerrhexis technique for small incision lenticule extraction. J Refract Surg. 2015;31:16-21.
[Crossref] [Google Scholar] [PubMed]
- Jacob S, Agarwal A, Mazzotta C, et al. Sequential segmental terminal lenticular side-cut dissection for safe and effective small-incision lenticule extraction in thin lenticules. J Cataract Refract Surg. 2017;43:443-8.
[Crossref] [Google Scholar] [PubMed]
- Ramirez-Miranda A, Ramirez-Luquin T, Navas A, et al. Refractive lenticule extraction complications. Cornea. 2015;34:S65-7.
[Crossref] [Google Scholar] [PubMed]
- Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121:822-8.
[Crossref] [Google Scholar] [PubMed]