Research Article - Journal of Clinical Ophthalmology (2025) Volume 9, Issue 1
Advances in intense pulsed light therapy for ocular surface disorders.
Ruida Chen1,2, Jie Zhou1,3, Haohan Zheng1, Yirui Zhu1*
1Department of Ophthalmology, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Zhejiang, China
2Department of Ophthalmology, Affiliated Dongyang Hospital, Wenzhou Medical University, Dongyang, China
3Department of Ophthalmology, Songyang Hospital of Traditional Chinese Medicine, Lishui, China
*Corresponding Author:
- Yirui Zhu
- Department of Ophthalmology, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Zhejiang, China
- E-mail: yiruizhu@zju.edu.cn
Received: 25-Nov-2024, Manuscript No. AACOVS-24-153220; Editor assigned: 28-Nov-2024, AACOVS-24-153220 (PQ); Reviewed: 12-Dec-2024, QC No. AACOVS-24-153220; Revised: 08-Apr-2025, Manuscript No. AACOVS-24-153220 (R); Published: 15-Apr-2025, DOI: 10.35841/aacovs.9.1.499
Citation: Chen R, Zhou J, Zheng H, et al. Advances in intense pulsed light therapy for ocular surface disorders. J Clin Ophthalmol 2025;9(1):503.
Abstract
Since its initial use in 2002 to treat Meibomian Gland Dysfunction (MGD) and Dry Eye Disease (DED), Intense Pulsed Light (IPL) therapy has evolved into a widely adopted treatment for various ocular surface diseases. This review examines the latest advancements in IPL therapy, with a focus on its emerging applications in conditions such as blepharitis, refractory dry eye, blepharitis-associated keratoconjunctivitis, glaucoma-related DED, chalazion and more. Key mechanisms underlying IPL's effectiveness, including microbial modulation, anti-inflammatory effects and photobiomodulation, are discussed. Furthermore, this review highlights innovations in IPL systems, such as the M22, E-Eye and EOS devices, which improve treatment precision and patient comfort. Clinical studies have demonstrated the significant efficacy of IPL in managing MGD, enhancing tear film stability, reducing symptoms of dry eye and even addressing complex cases like recurrent chalazion and chronic hordeolum. Notably, IPL has shown promising results when combined with other therapies, including diquafosol, cyclosporine and Meibomian Gland Expression (MGX), indicating its potential as a multimodal treatment approach. The review also explores IPL’s role in perioperative care for refractive surgery patients and as a therapeutic option for glaucoma-related dry eye. Despite the growing body of evidence supporting IPL's clinical utility, further large-scale randomized controlled trials are needed to better define its role in treating ocular surface diseases and to explore its full therapeutic potential.
Keywords
Keratoconjunctivitis, Chronic hordeolum, Blepharitis, Chalazion.
Introduction
Since 2002, when Toyo first identified the effects of Intense Pulsed Light (IPL) on Meibomian Gland Dysfunction (MGD) and Dry Eye Disease (DED), numerous studies have sought to refine the IPL procedure for managing DED. In recent years, IPL has also been employed to treat conditions such as blepharitis, refractory dry eye, Blepharitis-associated Keratoconjunctivitis (BKC), glaucoma-related DED and chalazion. These advancements have contributed to the widespread clinical adoption of IPL, which is now routinely administered as a multi-visit, in-office treatment in more than 50 countries. This review examines recent literature available in the PubMed database, focusing on the emerging applications of IPL in the treatment of ocular surface diseases [1].
Materials and Methods
Mechanism of IPL therapy
Eradication of Demodex and increases in bacterial community: Certain microbes, including Staphylococcus aureus, Bacillus oleronius and Demodex mites (D. folliculorum and D. brevis), release toxic substances such as lipases, which alter the lipid composition, increase viscosity and obstruct follicles and glands. This process triggers inflammatory mediators, including Metalloproteinase-9 (MMP-9). A previous study observed a reduction in the mean number of Demodex mites among patients following IPL treatment. Somboonna, et al. conducted metagenomic DNA analysis of eyelashes from both upper and lower eyelids of healthy participants and those with MGD, assessing samples before and after the second, third and fourth IPL treatments. Their findings revealed that bacterial diversity was higher in healthy individuals compared to severe MGD cases. Furthermore, the relative abundance of bacteria in MGD participants progressively resembled that of healthy individuals during the IPL sessions. This suggests that IPL treatment may reshape the eyelash microbiome in MGD cases. However, further research is needed to understand the microbiome’s role in MGD pathogenesis and its response to treatment [2].
Anti-inflammatory effects: A recent report indicates that levels of MMP-9 in tears significantly decrease after IPL treatment combined with the use of 0.05% cyclosporine eye drops in patients with MGD. Similarly, another study found that 0.05% cyclosporine alleviates dry eye symptoms via similar pathways. However, research on the exact mechanisms underlying the beneficial effects of IPL in the treatment of MGD is complex and limited. Notably, the anti-inflammatory mechanisms of IPL have yet to be directly validated in patients with ocular surface diseases [3].
Photobiomodulation and intracellular mechanisms: Reactive Oxygen Species (ROS) are key intermediates in photobiomodulation. After the absorption of light energy by chromophores such as opsin and water molecules, intracellular levels of mitochondria-derived ROS are modulated-either directly or indirectly via pathways such as ERK/FOXM1/c- Myc and MAPK. These pathways play a role in promoting cell differentiation and tissue regeneration in various microenvironments. Meanwhile, low-level laser therapies, such as IPL, have been shown to reduce ROS levels. This reduction influences the expression of enzymes such as calciumdependent Phospholipase A2 (cPLA2), secretory Phospholipase A2 (sPLA2) and Cyclooxygenase-2 (COX-2), ultimately inhibiting the release of Prostaglandin E2 (PGE2). While most evidence stems from dermatological and basic research, the intracellular mechanisms of IPL still require direct validation in patients with ocular surface diseases [4].
Results and Discussion
Updates on the clinical application of IPL therapy
Light-guided tip on different ipl systems: The M22 IPL system (Lumenis Ltd., Yokneam, Israel) utilizes a sapphirecooled, 6-mm cylindrical light guide with a fluence of 15-20 J/cm2. This design allows for safer, more precise and effective treatment by targeting smaller areas of the eyelid skin. Recently, the E-Eye IPL system (E-SWIN company, France) introduced enhancements such as delivering light pulses to four overlapping periocular zones below each eye and a fifth pulse anteriorly, along with the addition of a cylindrical light-guided tip. Similarly, the EOS IPL system (Medical Itabashi Company, Japan) has incorporated a cylindrical light-guided tip. The recommended energy for the E-Eye IPL The recommended energy for the E-Eye IPL is 9.0 J/cm2, whereas the EOS IPL system operates at a higher range of 15-22 J/cm2. The E-Eye IPL systems’ smaller guide head, characterized by its low energy output, painless treatment and ease of use, makes it particularly suitable for treating children with conditions such as Blepharokeratoconjunctivitis (BKC) and meibomian gland inflammation (Figure 1) [5].

Figure 1. Three different IPL light-guided tips.
IPL therapy for MGD: While most studies focus on the use of IPL in managing MGD, its efficacy has been increasingly explored in recent research. Patricia et al. explored the long-term effectiveness of IPL therapy for DED associated with MGD over a 1-year follow-up period. Key metrics, including eye fitness test scores and Noninvasive Breakup Time (NIBUT), were evaluated at follow-up intervals (3, 6 and 12 months), with IPL sessions conducted on days 1, 15, 45 and 75. The study reported significant improvements in both NIBUT and eye fitness scores across the entire 12-month period, indicating enhanced tear film stability and alleviation of subjective symptoms. These findings advocate for IPL therapy’s long-term efficacy in enhancing tear film stability and improving subjective symptoms of dryness, corroborating the inclusion of IPL therapy in the repertoire of treatment modalities for DED. At the same time, in a prospective, randomized, controlled trial, 44 eyes were treated with IPL combined with 3% diquafosol instead of Meibomian Gland Expression (MGX), while another 44 eyes were placed in a sham group. As a result, significant improvements in NIBUT, tear-film lipid layer, corneal and conjunctival staining, Meibomian Gland (MG) quality and expressibility, and ocular surface disease index were found in the IPL combined with 3%diquafosol therapy. Conversely, the sham group showed no notable improvements. These results highlight the superior efficacy of IPL combined with 3% diquafosol therapy compared to IPL alone for alleviating the signs and symptoms of severe MGD [6].
IPL therapy for chalazion and chronic hordeolum:
Recurrent chalazion is considered a pathognomonic localized form of MGD characterized by lid margin abnormalities, such as plugging, vascularity of orifices and a large loss of MGs. In 2022, we enrolled patients whose chalazion had failed to resolve after repeated traditional surgeries. These patients underwent IPL and MGX sessions on days 1, 15, 45 and 75 until the lesion resolved. Four weeks after the final treatment, significant improvements were observed in TBUT, meibum quality and expressibility scores. In addition, the combined IPL-MGX treatment resulted in a very low recurrence rate, even after an average of just four treatments. A similar conclusion was reached by Yoon, et al. In their study, doxycycline was combined with IPL therapy instead of MGX in 12 patients with refractory recurrent chalazion. Significant improvements were noted in the MG expression scores, MG quality scores and lid margin vascularity scores. Recently, our group investigated a novel technique involving repeated light- guided IPL treatments combined with MGX for recurrent or refractory chalazion. The protocol included two IPL steps: The administration of 12 IPL pulses to the upper and lower eyelid perpendicular regions, followed by 6-10 pulses around each chalazion using a light-guided tip. This technique was found to be an efficient therapy for reducing the size and recurring frequency of chalazion, as well as for improving MG function (Figure 2). These findings suggest that IPL combined with MGX could be considered a first-line treatment for primary or recurrent chalazion with inflammation [7].
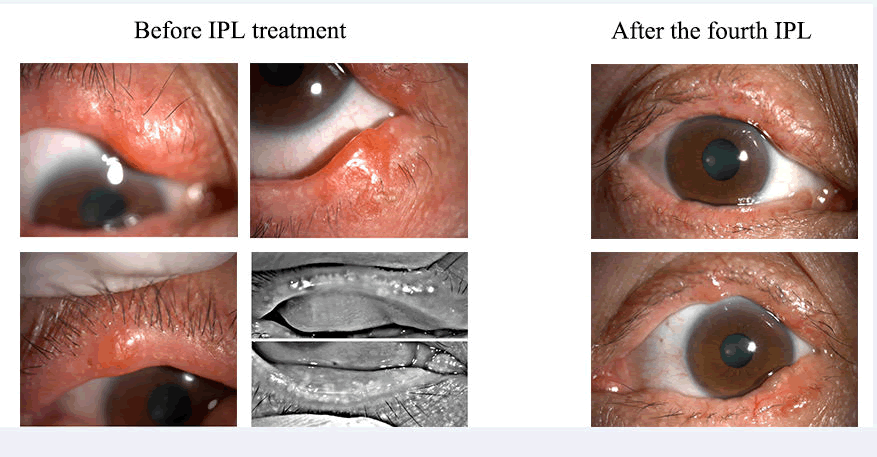
Figure 2. Comparison of a typical patient with recurrent and multiple chalazion before and after the fourth IPL treatment.
Unlike chalazion, hordeolum is a common inflammatory eyelid condition that affects the MG or the glands of Zeis or Moll. Ke Yang, et al. evaluated the effects of IPL treatment on chronic hordeolum. Their study found significant reductions in visual analog scale scores for pain, eyelid congestion and nodule size. Additionally, improvements were observed in eyelid margin signs, MG quality and expression, tear meniscus height and corneal fluorescein staining scores. These findings suggest that IPL is a safe and effective treatment option for managing hordeolum [8].
Perioperative IPL for refractive surgery: Studies have evaluated IPL postoperative use in patients following Laser- Assisted in situ Keratomileusis (LASIK) surgery, with successful outcomes observed in patients up to 10 years postsurgery. Martínez-Hergueta, et al. considered the use of perioperative IPL as a prophylactic therapy for ocular surface disorders. In this clinical trial with 61 patients who were randomized into two groups, IPL sessions were applied 7 days before, 7 days after and 21 days after the refractive procedure. Ocular Surface Disease Index (OSDI), NIBUT and MG quality and expressibility were significantly improved. These findings indicate that perioperative IPL therapy applied to laser corneal refractive surgery improves objective and subjective ocular surface parameters and effectively prevents dry eye symptoms during the early postoperative period [9].
IPL for glaucoma-related dry eye: Due to the chronic use of topical anti-glaucoma drugs, glaucoma-related DED is frequently seen in eye clinics. As patient adherence to drugs for the treatment of glaucoma and subjective complaints in dry eye can be negatively affected by the addition of topical ocular lubricants such as hyaluronic acid, non-drug therapies like IPL seem particularly important. In a study, one eye of each participant-who refrained from using any dry eye treatments or eye drops during the study-was randomly assigned to either an IPL or a control group. In the IPL group, significant improvements were observed in NIBUT, tear meniscus height, corneal fluorescein staining, tear-film lipid layer, MG expressibility, and OSDI. Zhang, et al. proposed that IPL therapy could serve as an alternative to topical antibiotics (to reduce bacterial load), steroids or cyclosporine for mitigating inflammation. This approach could also actively improve patient adherence to anti-glaucoma medications by addressing dry eye symptoms more effectively.
Conclusion
Based on current literature, we conclude that IPL, when combined with other treatment modalities, significantly improves outcomes in various ocular surface diseases. Increasing evidence indicates that IPL is an effective treatment modality for MGD, DED after refractive surgery, glaucomarelated dry eye, Demodex infestation and recurrent chalazion. Larger randomized controlled trials evaluating the effectiveness of IPL for these diseases are required to explore the full potential of IPL. Given the excellent efficacy and safety profile of IPL, its potential as a treatment for ocular surface conditions other than those considered herein should be investigated.
References
- Cote S, Zhang AC, Ahmadzai V, et al. Cochrane eyes and vision group. Intense Pulsed Light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev. 1996;3:CD013559.
[Crossref] [Google Scholar] [PubMed]
- Qin Z, Zhu Y, Lu J, et al. Therapeutic effectiveness of different machines in intense pulsed light treatment of meibomian gland dysfunction. Adv Ophthalmol Pract Res. 2024;4:182-8.
[Crossref] [Google Scholar] [PubMed]
- Dong Q, Brulc JM, Iovieno A, et al. Diversity of bacteria at healthy human conjunctiva. Invest Ophthalmol Vis Sci. 2011;52:5408-13.
[Crossref] [Google Scholar] [PubMed]
- Cheng SN, Jiang FG, Chen H, et al. Intense pulsed light therapy for patients with meibomian gland dysfunction and ocular Demodex infestation. Curr Med Sci. 2019;39:800-9.
[Crossref] [Google Scholar] [PubMed]
- Somboonna N, Wongsaroj L, Watthanathirakawi A, et al. Potential impact of ocular intense pulsed light on eyelash microbiome in severe meibomian gland dysfunction: Report of 2 cases. Front Ophthalmol. 2023;3.
[Crossref] [Google Scholar] [PubMed]
- Jeon YY, Bae S, Chung HS, et al. Effects of combined intense pulsed light and cyclosporine 0.05% eyedrops in ocular surface matrix metalloproteinase-9 levels in patients with moderate-to-severe MGD. Lasers Med Sci. 2024;39:203.
[Crossref] [Google Scholar] [PubMed]
- Nussenblatt RB, Palestine AG. Cyclosporine: Immunology, pharmacology and therapeutic uses. Surv Ophthalmol. 1986;31:159-69.
[Crossref] [Google Scholar] [PubMed]
- Ramzan R, Vogt S, Kadenbach B. Stress-mediated generation of deleterious ROS in healthy individuals-role of cytochrome c oxidase. J Mol Med. 2020;98:651-7.
[Crossref] [Google Scholar] [PubMed]
- Chen CH, Wang CZ, Wang YH, et al. Effects of low-level laser therapy on M1-related cytokine expression in monocytes via histone modification. Mediators Inflamm. 2014;2014:625048.
[Crossref] [Google Scholar] [PubMed]