Research Article - Biomedical Research (2018) Volume 29, Issue 20
Morphological study of Hyrtl's anastomosis in gestational diabetes mellitus and its relation to umbilical cord insertion
Seema Valsalan E1*, Ramakrishnan PK1, Chitra S2, Senthil Kumar S3, Sruthi MV4, Akshara VR1 and Benjamin W1
1Department of Anatomy, P K DAS Institute of Medical Sciences, Vaniamkulam (PO), Palakkad (District), Kerala, India
2Department of Pathology, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences, Thandalam, Chennai, Tamil Nadu, India
3Department of Anatomy, SRMC, Porur, Chennai, Tamil Nadu, India
4Department of Community Medicine, Amala institute of Medical Sciences, Thrissur, Kerala, India
- *Corresponding Author:
- Seema Valsalan E
Department of Anatomy
P K DAS Institute of Medical Sciences
Kerala, India
Accepted date: October 29, 2018
DOI: 10.4066/biomedicalresearch.29-18-971
Visit for more related articles at Biomedical ResearchAbstract
Gestational diabetes mellitus having a great effect on the structure of the umbilical cord vessels can affect the hemodynamic in these vessels and bring variations in the anastomotic pattern of umbilical arteries and mode of umbilical cord insertion. Hyrtl’s anastomotic pattern and its correlation to cord insertion has so far not been studied in umbilical cords of GDM mothers. Hence, a study on Hyrtl’s anastomosis in GDM and normal pregnancy helps to understand the anatomy exhibited by the different groups and to add to the already existing quantum of knowledge. 59 GDM and 52 normal umbilical cords attached to placenta were procured from the operation theatre and labour room, department of Obstetrics and Gynaecology of PK Das Institute of Medical Sciences and Research, Palakkad. Our study reveals that the characteristics of Hyrtl’s anastomosis differ in the umbilical cords of GDM mother from that of normal mothers by adopting anastomosis by branching pattern and there do not exists a correlation between the Hyrtl’s anastomosis and cord insertion in both groups.
Keywords
Hyrtl’s anastomosis, Umbilical arteries, Cord insertion
Introduction
Embryo receives its nutrition from tubal and uterine secretions followed by fluid filled cavities of amnion, coelom and yolk sac. Later as these sources are diminished and therefore become imperative that some other sources are available. This brings the maternal circulation into close, although indirect, opposition with embryonic circulation by the development of umbilical cord and placenta. The umbilical cord has 2 umbilical arteries to carry poorly oxygenated blood to the placenta and to carry oxygenated blood from placenta back to the embryo there is one umbilical vein which maintain the fetomaternal circulation and becomes the lifeline of the foetus [1]. In the early gestation multiple anastomosis occur between the umbilical arteries that is subsequently reduced to one [2,3]. This is due to the discordant blood flow pattern in the umbilical arteries at the time of development. It is learned to be diminished as the pregnancy advances indicating the functional maturation of Hyrtl’s anastomosis with the increasing gestation [4]. Between the two umbilical arteries, Hyrtl’s anastomosis is the only connection within the first 2 to 3 cm of cord proximal to the chorionic plate [5]. The main function of Hyrtl’s anastomosis is to balance the pressure and flow in the two umbilical arteries helping to equalize the area of placental vascular territories [5,6]. Computer modelling studies had enabled to understand its regulating role in the blood flow and its distribution to the placenta [7]. Perfectly symmetrical umbilical arteries may lack anastomosis [8]. The anatomy of Hyrtl’s anastomosis is the main factor determining the area of supply by the umbilical arteries [9]. In case of partial compression of placenta it is considered as a safety valve that may occurs during uterine contraction or occlusion of an umbilical artery and its absence could be responsible for the incident of discordant umbilical arteries, which is often associated with placental anomalies like velamentous, marginal insertion and infarct [10]. Single umbilical artery and fusion of umbilical arteries also show high prevalence of velamentous, marginal cord insertion and asymmetrical placental lobes [11,12]. No difference was observed in anastomotic pattern and anastomotic diameter of Hyrtl’s anastomosis in AGA and SGA fetus indicates that the presence and function of Hyrtl’s anastomosis depends on the placental morphology [13]. It was suggested that linking any factor to the presence or absence of the anastomosis was impossible. Further, in a study where differences in the area of the placenta served by the arteries were present, the arteries were found to be of equal size in the presence of the anastomosis [14,15].
Most commonly the umbilical cord inserts centrally or eccentrically (>90%) and are not associated with pathology. Marginal, velamentous and furcated insertions have important clinical consequences [15,16]. After the insertion of placental cord, umbilical arteries get separated and supply only one placental lobe. Each of the arteries further get divided into the several end-placental arteries which end at the centre of the placental cotyledons. Usually two umbilical arteries possess similar diameter. Any discordance in the diameters of the arteries is associated with abnormalities in placenta, dissimilarities in umbilical cord insertion and few clinical conditions, like gestational diabetes mellitus [13]. But some authors couldn’t find any relation with discordant umbilical arteries with placental and cord abnormalities [17]. Gestational diabetes mellitus having a great effect on the structure of the umbilical cord vessels which can affect the hemodynamic in these vessels and bring variations in the anastomotic pattern of umbilical arteries and mode of umbilical cord insertion [18]. Hyrtl’s anastomotic pattern and its correlation to cord insertion has so far not been studied in umbilical cords of GDM mothers. Hence, a study on Hyrtl’s anastomosis in GDM and normal pregnancy helps to understand the anatomy exhibited by the different groups and to add to the already existing quantum of knowledge.
Materials and Methods
Study setting
The Study was conducted in the department of Anatomy in P K.DAS Institute of Medical Sciences and Research, Palakkad.
Study participants
After ethical approval from institutional ethical committee, 59 GDM and 52 normal umbilical cords attached to placenta were procured from the operation theatre and labour room, department of Obstetrics and Gynaecology of P.K.DAS Institute of Medical Sciences and research, Palakkad. History was taken from medical records to differentiate between normal and GDM.
Inclusion criteria
52 mothers with normal pregnancy and 59 mothers with pregnancy complicated by GDM confirmed according to the present criteria of the American Diabetic Association following normal vaginal deliveries or caesarean section.
Exclusion criteria
Women having any other pathological abnormalities like preeclampsia, eclampsia, heart, liver, renal diseases, endocrine disorders, malignancies and in normal pregnancies mothers having familial history of diabetes is excluded.
Methodology
Specimens were washed and cleaned to remove blood and mucus. After noting the mode of insertion to placenta specimens were preserved in 10% formaline. After 3-4 d of fixation longitudinal dissection of the umbilical cord 10 cm proximal to the placenta was done to expose the umbilical arteries and vein. The differences in the anastomotic pattern of umbilical arteries were observed and compared among normal and GDM and correlated with umbilical cord insertion.
Ethical considerations
The present study was approved by institutional ethical committee. IEC No-IEC/12-2/2015.
Data analysis
Data was analysed by using SPSS 20.0. Data was expressed as frequency and percentage. Fischer’s exact test was applied to observe the association. P value less than 0.05 was considered as significant.
Results
Results were presented in Tables 1 and 2. Total 111 pregnant mothers were included in the study. Out of 111 pregnant mothers 59 had GDM and 52 were normal pregnancies. The mean age of pregnant mothers was 26.13+4.71 with minimum age 19 and maximum 44 y. Upon examination of 111 umbilical cords, all five types of previously described anastomosis were observed as shown in Table 1: transverse (Figure 1A), oblique (Figure 1B), fenestrated (Figure 1C), fused (Figure 1D), and anastomosis by branches (Figure 1E). In addition, we also observed one specimen having double anastomosis (Figure 1F) and 2 cases lacked anastomosis (Figure 1G). In spite of finding all types of anastomosis in umbilical cords in both normal and GDM mothers, the distribution was varied. The fenestrated and transverse types were equally common in normal cases (60.9% and 65.4%, respectively). In contrast, in GDM cases, anastomosis by branches was found more prominent (78%), a 3-4 fold difference from normal was observed (Table 2). There is statistically significant difference between GDM and normal Hyrtl’s anastomosis (p-value=0.003) fused anastomosis was less in GDM compared to normal mothers (1 vs. 3), but the fractions of oblique and no anastomosis were similar in the two groups. No cases of a single artery were observed in each group. In addition to this, we found a double anastomosis in one of the cases of GDM. The umbilical arteries were connected to each other by two transverse anastomosis. Of 111 cases investigated, 52 of normal and 59 of GDM, all the types of known insertions like central, eccentric, marginal, velamentous and furcate was observed. The commonest insertion found was eccentric 30 (60%) in GDM and 20 (40%) in normal, followed by central 19 (42.2%) in GDM and 26 (57.8%) in normal. Marginal insertion was 6 (50%) in GDM and 6 (50%) in Normal. Velamentous 3 (100%) and furcate 1 (100%) insertions were found only in GDM. On comparison no significant difference was observed among the two groups (Fischer’s exact value was 8.21 and P value was 0.08). When Association between umbilical cord insertion site and Hyrtl’s anastomosis was observed, there was no significant correlation between them (Fischer’s exact value was 23.41 and P value was 0.495).
| Type of Hytrl’s anastomosis | Figure 1. | Number | Percentage |
|---|---|---|---|
| Transverse | 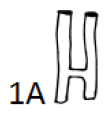 |
23 | 20.7% |
| Oblique | 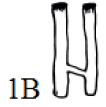 |
14 | 12.6% |
| Fenestrated | 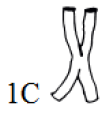 |
26 | 23.4% |
| Fused | 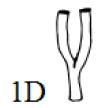 |
4 | 3.6% |
| Anastomoses with branches |  |
41 | 36.9% |
| Double anastomoses |  |
1 | 0.9% |
| No anastomoses |  |
2 | 1.8% |
| Total | 111 | 100% |
Table 1. Type of Hyrtl’s anastomosis. (Data presented was frequency and percentage).
| Hytrl’s anastomoses | Umbilical cord | Total | Statistical significance | |
|---|---|---|---|---|
| GDM | Normal | |||
| Transverse | 9 (39.1%) | 14 (60.9%) | 23 | Fischer’s exact value-19.55; P value-0.003* |
| Oblique | 6 (42.9%) | 8 (57.1%) | 14 | |
| Fenestrated | 9 (34.6%) | 17 (65.4%) | 26 | |
| Fused | 1 (25%) | 3 (75%) | 4 | |
| Anastomoses with branches | 32 (78.1%) | 9 (21.9%) | 41 | |
| No anastomosis | 1 (50%) | 1 (50%) | 2 | |
| Double anastomoses | 1 (100%) | 0 | 1 | |
| 59 | 52 | 111 | ||
Table 2. Comparison of Hytrl’s anastomosis among umbilical cord of GDM and normal pregnancy (Chi-square test is used and P value less than 0.05 is significant).
Discussion
Anastomosis between the umbilical arteries was not investigated in the GDM cases. Hence, we examined specimens from normal and GDM mothers. Anastomosis were learned to be present in the umbilical arteries close to the cord insertion [19]. The present study also identified similar features in all the specimens collected. Earlier studies illustrated that the umbilical arteries possess single connection in connecting all the arteries and were never connected by two or more anastomosis [20]. Literature showed two anastomosis in a specimen and this was found only in one case till date wherein a double anastomosis was reported in one among 200 cases investigated [21,22]. In the present study we found a single case of double anastomosis in accordance to the previous studies. The earlier investigations mentioned various types of Hyrtl’s anastomoses like transverse, oblique, fused, anastomosis by branches, double and no anastomosis characterized by using different techniques like the Doppler method, injection corrosion technique and angiography [23,24]. In many of the studies conducted previously on Hyrtl’s anastomosis transverse anastomosis was common, but there was no information whether the studies were conducted on normal or pathologic placenta [6,25,26]. The median diameter of the Hyrtl’s anastomosis was found significantly higher when the anastomosis was oblique than transverse [27].
In the present study out of 111 cases anastomosis was present in 109 cases. The commonest types of anastomosis in normal was fenestrated 17 (65.4 %) followed by transverse 14 (60.9%), anastomosis by branches 9 (21.9%), oblique 8 (57.1%) and fused 3 (75%). In GDM the anastomosis by branches 32 (78.1%) was found to be significantly higher, followed by transverse 9 (39.1%), fenestrated 9 (34.6%), oblique 6 (42.9%) and fused 1 (25%). Anastomosis was absent in 2 cases, one from each group and there was no single umbilical artery in both study group. A double anastomosis was observed in one GDM case where the umbilical arteries were connected by two transverse anastomosis.
Karma et al. studied Hyrtl’s anastomosis in pregnancy induced hypertensive placentae and observed all types of Hyrtl’s anastomosis with transverse being more prominent in pregnancy induced hypertension [22,28]. The thickness of tunica media was found to be more in umbilical arteries and Hyrtl’s anastomosis of hypertensive patients [29].
Hyrtl’s anastomosis was found normal in small for gestational age foetus and its static measurements were not contributing for the same [9]. Adoption of Hyrtl’s anastomosis by GDM mothers if fails to overcome the resistance and pressure difference between the arteries to supply the placental territories equally may lead to abnormal insertions. So the present study investigated a correlation between the cord insertion and Hyrtl’s anastomosis in GDM and the present study couldn’t find any correlation between these as all types of insertions were almost equally distributed among each Hyrtl’s type. GDM has heavy toll on vascular structure of umbilical cords and placenta affecting the hemodynamic of fetoplacental circulation. The present study investigated the morphological pattern of Hyrtl’s anastomosis in umbilical cords derived from normal versus GDM mothers.
Conclusion
Our study reveals that the characteristics of Hyrtl’s anastomosis differ in the umbilical cords of GDM mothers from that of normal mothers by adopting anastomosis by branching pattern and there is no correlation between the Hyrtl’s anastomosis and cord insertion in both groups.
Limitations
Longitudinal dissection was done only for 5-10 cm proximal to placenta as the remaining part of the cord was needed for histological study.
References
- Gray H, Standring S, Ellis H, Berkovitz B. Grays anatomy (39th Edn.). Edinburgh: Elsevier Churchill Livingstone 2005.
- Stieve H, Strube J. Uber Die Entwicklung des Dotter sackreislaufesbrim Menschen Ztschr, Mikroskop. Anat Forsch 1933; 32: 107-173.
- Patten BM. Human Embryology. Philadelphia: Blakistan Company 1946.
- Predanic M, Kolli J, Yousefzadeh P, Pennisi J. Disparate blood flow patterns in parallel umbilical arteries. Obstec Gynecol 1998; 91: 757-760.
- Hyrtl J. Blutgef€asse der MenschlichenNachgeburt in NormalenundAbnormenVerh€altnissen.Braum€ullerVerlag, Vienna 1870.
- Bacsich P, Smout. Some observations on the foetal vessels of the human placenta with an account of the corrosion technique. JAnat 1938; 72: 358-361.
- Gordon Z, Eytan O, Jaffa AJ, Elad D. Hemodynamic analysis of Hyrtl anastomosis in human placenta. Am J Physiol Regul Inter Comp Physiol 2006; 292: 977-982.
- Ullberg U, Sandstedt B, Lingman G. Hyrtls anastomosis, the only connection between the two umbilical arteries. A study in full term placentas from AGA infants with normal umbilical artery blood flow. Acta Obstet Gynecol Scand 2001; 80: 1-6.
- Ullberg U, Goran L, Gunvor E, Hyrtls anastomosis is normally developed in placentas from small for gestational age infants. Acta Obstet Gynecol Scand 2003; 82: 716-721.
- Dolkart LA, Reimers FT. Discordant umbilical arteries: ultrasonographic and Doppler analysis. Obstet Gynecol 1992; 79: 59-63.
- Raio L, Ghezzi F, Di Naro E, Franchi M, Bruhwiller H. Prenatal assessment of the Hyrtl anastomosis and evaluation of its function. Human Reprod 1999; 14: 1890-1893.
- Fujikura T. Fused umbilical arteries near placental cord insertion. Am J Obstet Gynecol 2003; 188: 765-767.
- Raio L, Ghezzi F, Di Naro E, Gomez R, Salee G, Bruhwiler H. The clinical significance of antenatal detection of discordant umbilical arteries. Obstet Gynecol 1998; 91: 86-91.
- Young A. The primate umbilical cord with special reference to the transverse communicating artery. J Hum Evol 1972; 1: 345-359.
- Benirsschke K, Kaufmann P. Pathology of the human placenta.4th Ed. Anatomy and Pathology of the umbilical cord and major fetal vessels. Springer New York 2000; 335-398.
- Robinson LK, Jones KL, Benirschke K. The nature of structural defects associated with velamentous and marginal insertion of the umbilical cord. Am J Obstetr Gynecol 1983; 146: 191-193.
- Sepulveda W, Flack NJ, Bower S, Fisk NM. The value of color Doppler ultrasound in the prenatal diagnosis of hypoplastic umbilical artery. Ultrasound Obstet Gynecol 1994; 4: 143-146.
- Kumar, V Robbins, SL. Robbins basic pathology (8th Edn.). Philadelphia PA: Saunders/Elsevier 2007.
- Hebenstreit E. Funiculiumbel pathologia. Lips 1737.
- Shordania J. Uber das Gefassystem der NabelschnurZtsch. FAnat U Entwicklgsch 1929; 89: 696-726.
- Priman J. A note on the anastomosis of the umbilical arteries. Anat Rec 1959; 134: 1-5.
- Bhutia KL, Sengupta R. Pregnancy-induced hypertension is associated with altered anatomical patterns of Hyrtls anastomosis. Anatomic Rec 2014; 297: 819-825.
- Arts NF. Investigations on the vascular system of the placenta. Am J Obstet Gynecol 1961; 82: 147-158.
- Seo KA, Kim MJ. Patterns of Hyrtls anastomosis and their effects on Ostetric out comes. Korean J Obstet Gynecol 2004; 47: 83-90.
- Szpakowski M. Morphology of arterial anastomoses in the human placenta. Folia Morphol 1974; 33: 53-60.
- Salfia C, Popek E. Mechanical pathophysiology of the placenta. Glob Libo womens Med 2008; 107: 1-7.
- Raio L, Ghezzi F, di Naro E, Franchi M, Balestreri D, Dürig P. In-utero characterization of the blood flow in the Hyrtl anastomosis. Placenta 2001; 22: 597-601.
- Bhutia KL, Sengupta R. Morphological study in Hyrtls anastomosis of umbilical arteries in pregnancy-induced hypertension. J Anat Soc India 2013; 62: 37-39.
- Bhutia KL, Sengupta R, Kanungo BK, Upreti, B, Tewari J, Tamang BK. Image J analysis of tunica media of Hyrtls anastomosis in pregnancy induced hypertension. GSTF J Adv Med Res 2014; 1: 2.